Suicide in Norway
Last update
|Two out of three who die as a result of suicide are men. Many relatives and close friends are affected by suicide every year.

Main points
- Approximately 650 people die as a result of suicide every year in Norway. Two out of three are men.
- The number of suicides per 100,000 inhabitants has declined since 1990, but is still higher than in the 1950s and 60s.
- The median age of suicide is 47 years, which means that half are older and half are younger than 47 years.
- Approximately 6500 bereaved family members and close friends are affected by suicide every year.
- The incidence of suicide in Norway is similar to Europe, North America and Australia.
About suicide, suicide attempts and self-harm
Suicide is the result of a self-inflicted injury with the intent to end life.
Suicide attempts and self-harm are usually different phenomena.
- In the case of suicide attempts, there is an intention to die, although the intention may vary in strength.
- Self-harm is not necessarily associated with a desire to die, but rather an expression of a way to regulate intense negative thoughts, painful emotions or a difficult relationship (Øverland, 2006).
Data source and glossary
Suicide statistics are extracted from the Norwegian Cause of Death Registry. Deaths are coded as suicides in the registry if suicide/ probable suicide was reported on the death certificate or the post-mortem report.
There is sometimes some degree of uncertainty concerning the registration of suicide. Some suicides are categorised incorrectly as accidents. There is also a grey zone between accidents and suicide. Lack of information about the reported cause of death can also hinder correct registration in the Cause of Death Registry.
In the case of suicide attempts and self-harm, there are no national figures for incidence and trends over time.Suicide rate
In order to compare the number of suicides over time, or between different populations, we must account for changes in the population. For this we use the suicide rate, which is the number of suicides per 100,000 inhabitants.
In addition, a correction is often made to account for different age distributions in the groups to be compared (age adjustment).
Median age
This age divides the group into two equal parts, meaning that there are as many people younger than this age as people who are older.
Suicide in Norway - status and trends
In 2021 there were 658 suicides registered in Norway, 482 men and 176 women (NIPH, 2022a). This figure is in line with 2018 and 2019, and somewhat higher than 2020. It is within the range of expected variation caused by random year-to-year fluctuations.
Trends over time
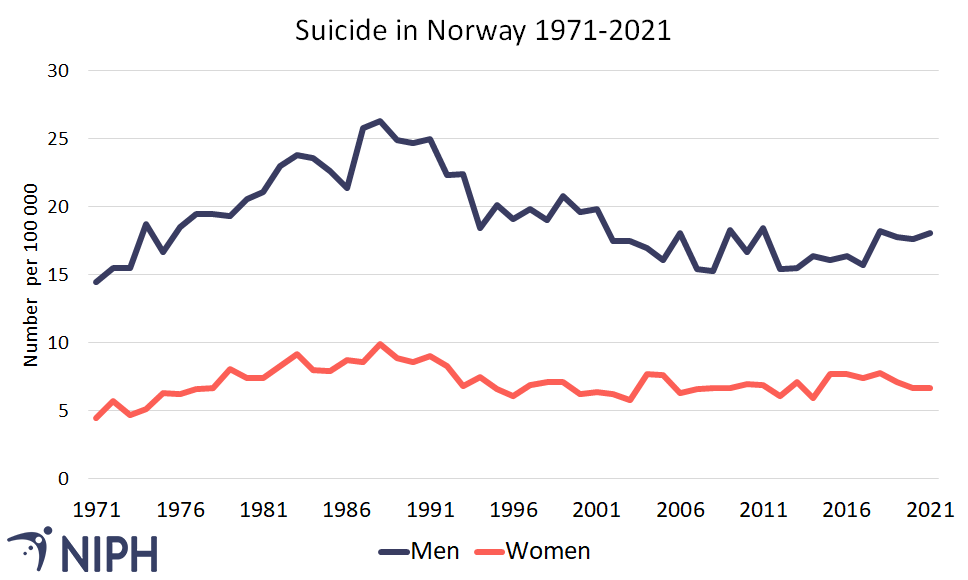
From 1970 to 1990, the incidence of suicide doubled but has since declined. The increase in suicides was most prominent among men aged 15 to 24 years. In 2021, the suicide rate was 12.4 per 100,000 inhabitants, which is about 25 per cent lower than in 1990 when the rate was 16.4 per 100,000 inhabitants (NIPH, 2022a). There has been a slight but significant increase in the age-standardised suicide rate between 2010 and 2019 (Raknes & Sveen, 2022). The rate for 2021 is as expected based on this development.
The decline in suicides from 1990 can primarily be attributed to a reduction in the number of suicides among men. For women, the decline in suicides continued until 1995 and since then, the rate has been relatively constant. For men, the decline continued before levelling off in recent years. Even though the suicide rate is lower now than in the 1990s, it is still considerably higher than before 1960.
The gender difference has become smaller; at the beginning of the time period there were almost three times as many suicides among men as among women, while the ratio is now approaching 2:1, see Figure 1.
For women, suicide rates for 2015 until 2019 were slightly higher than in recent years, but no more than could be expected with random fluctuations. The suicide rate for women was slightly lower in 2020 than between 2015 and 2019. There will always be some fluctuations in the number of suicides (and thus the suicide rate) from year to year. This is usually due to random variation.
Suicide methods have changed over time. Among men, hanging and suffocation are the most common methods, followed by the use of firearms. The proportion of people using this method has declined over the last 20 years. Among women, poisoning is as common as hanging or suffocation.
Suicide in different age groups
The median age of suicide was 47 years in 2020 (NIPH,2017).
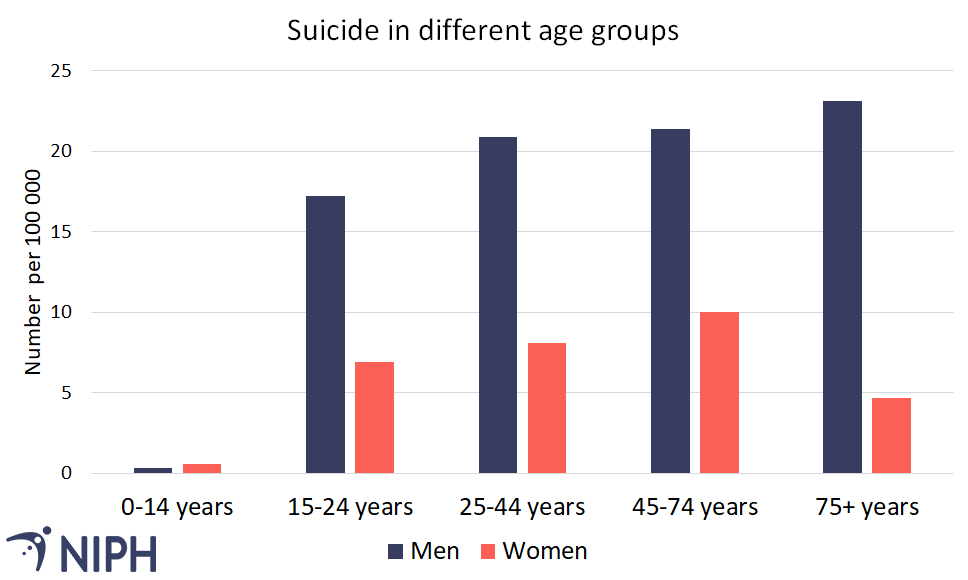
The suicide rate is higher for men than for women in all age groups when we exclude the youngest age group, see Figure 2.
- Suicide has very low prevalence in the youngest age group (0-14 years).
- In the 25 to 74 year-old age group, there are about 21 suicides among men per 100,000 inhabitants per year, while the rate for women is approximately 9 suicides per 100,000 inhabitants.
- Among the eldest, the number per 100,000 inhabitants is significantly higher among men than among women.
Trends during the COVID-19 pandemic in 2020 and 2021
During the pandemic, there has been concern about whether the lockdown of society with subsequent social isolation would have negative consequences on mental health and the risk of suicide in the population.
Analyses based on data from the Cause of Death Registry show that there was no increased incidence of suicide in any age group in 2020, and that the incidence was not higher during periods with particularly strict measures (Stene-Larsen et al., 2022).
County differences
Many counties in Norway have small populations and few suicides causing the random annual fluctuations to appear large. A few suicide deaths in a county can result in a large statistical difference. This makes the uncertainty around the suicide rate in each county high and it can be difficult to interpret whether a county actually has higher or lower suicide rates compared to the rest of the country.
International differences
From 1969-2000, there were major differences in the incidence of suicide between the Nordic countries. Today, the incidence is relatively similar in Norway, Sweden and Denmark (around 11 per 100,000 inhabitants), but Finland still has a significantly higher incidence than the other Nordic countries (almost 20 per 100,000).
The incidence of suicide in Norway resembles the rest of Europe, North America and Australia. In Europe, the average suicide rate was 11.7 per 100,000 for both sexes in the years 2006-2014 (European Commission, 2017). This is very close to the figures for Norway. However, there are even greater gender differences in the rest of Europe than in Norway. Compared with Norway, the figures are lower for women and higher for men. If using Eurostat, please note that the figures may differ from those in the Norwegian statistical banks because the statistics may be adjusted according to different age groups in the population.
In Eastern Europe, Russia, China, Japan and other countries in Asia with reliable statistics, the figures are higher than in Norway; 20-30 suicides per 100,000 inhabitants per year (Varnik, 2012). In these areas, suicide rates in most countries are higher among men than among women.
Consequences for the bereaved
Suicide has significant consequences for close family and friends, and for society as a whole. If we estimate that there are 10 bereaved people per suicide, approximately 6500 people are affected by suicide in Norway every year.
Several studies have found higher rates of post-traumatic stress reactions, prolonged grief, depression, anxiety and suicidal thoughts and / or suicide attempts among the suicide bereaved (Dyregrov, 2003; Groot, 2006; Pfeffer, 1997). Corresponding mental and physical problems have also been observed among the bereaved after other sudden deaths (Li, 2003). However, those who are bereaved by suicide report higher levels of feelings of rejection, shame, stigma and the need to conceal what has happened (Sveen, 2008).